
In Part 1 of this article, we introduced Medicare and its covered services, along with rationales for digital health startups to engage with the nation’s largest payer. These motivations include Medicare’s large and growing beneficiary base, access to the nation’s largest and most influential payer, and movement toward value-based care.
Despite these opportunities, startups have been relatively slow to service the Medicare space, instead choosing to focus on employers, commercial payers and direct-to-consumer offerings. We hypothesize one reason for the delayed entry is Medicare’s complex, rigid structure and stringent reimbursement regulations.
In Part 2 of this article, we brainstorm ways that early-stage companies can penetrate the Medicare market. We highlight several early-stage companies, many VC/PE backed, that have seen meaningful traction in the Medicare market. In keeping with our framework in Part 1 we describe each startup in the context of which part of Medicare the company serves: Parts A and B of Original Medicare (OM), Part C or Medicare Advantage (MA), and finally Part D, the prescription drug plan. Finally, we offer recommendations for emerging startups seeking to innovate in Medicare.
Key industry stakeholders
There are a handful of key Medicare industry stakeholder roles startups will either embody or interact with when delivering products or services to the Medicare population. We feel it’s important to understand these profiles and their incentives when positioning in the Medicare market.
Institutional providers and facilities
Providers include hospitals, skilled nursing facilities (SNF), home health agencies (HHA), clinics, opioid treatment programs and other institutional providers that have entered provider agreements under Medicare. Providers must submit an application to enter a Medicare-approved patient care services agreement.
Startups often deliver software and services to Medicare providers, who then pay these startups fees which are a small fraction of Medicare services revenues. Some startups will assume the costs and other regulatory requirements and apply for Medicare provider status themselves.
Payers
While the Centers for Medicare and Medicaid (CMS) is the payer for OM, Medicare’s ecosystem involves other payers and at-risk entities, such as MA plans. MA plans that seek to offer insurance products to Medicare-eligible patients must submit a Notice of Intent to Apply two years ahead of entering the market. The MA plan application itself is heavily scrutinized, and, once approved, MA plans must continue to meet Part C reporting requirements.
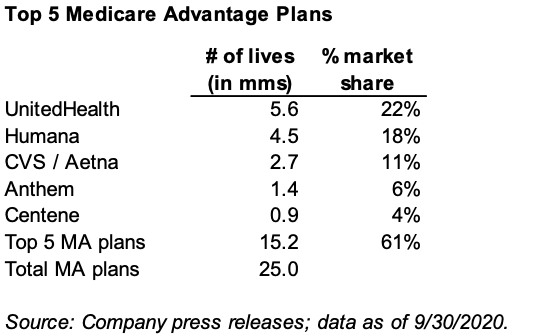 MA plans are an attractive customer for startups, given their value-based model and financial incentives to provide cost-effective care. In addition, several well-capitalized startups have launched as MA plans themselves, competing directly with a small set of dominant competitors that make up more than 60% of MA market share.
MA plans are an attractive customer for startups, given their value-based model and financial incentives to provide cost-effective care. In addition, several well-capitalized startups have launched as MA plans themselves, competing directly with a small set of dominant competitors that make up more than 60% of MA market share.
Suppliers and individual providers
Part B “suppliers” include physician and non-physician practitioners, clinics/group practices, and certain other suppliers who meet specific eligibility criteria. (See specific supplier hyperlinks.) Suppliers providing Durable Medical Equipment, Prosthetics, Orthotics and Supplies (DMEPOS) must be enrolled as an accredited organization, meet Part B quality standards and submit a surety bond. Startups may support these suppliers in providing software and care coordination services or serve as suppliers themselves.
Beneficiaries
While most startups have customer relationships with payers and providers, often the end user is the beneficiary or patient. In addition to being physically invested in Medicare services, beneficiaries also have financial motivations due to out-of-pocket financial responsibility for a portion of the cost of Medicare services. Most importantly, beneficiary engagement and participation in startup vendor or health plan programs are critical to demonstrating impact and value creation.
The startup landscape, organized by Medicare Parts
In the below sections, we profile digital health companies serving Medicare industry stakeholders, categorized by the part of Medicare they are addressing (Parts A-D). We also review financial incentives in Medicare and how startups can leverage them.
Medicare Part A
Startups innovating in the Medicare Part A space impact acute or post-acute care. This care is delivered by hospitals and skilled nursing facilities (SNF), as well as post-discharge home care delivered by Home Health Agencies (HHAs).
Hospitals are categorized as providers and paid through a fixed payment model called diagnosis-related groups (DRG). DRGs are shorthand for the average resources needed to treat a Medicare inpatient for a specific clinical condition. Hospitals received $137 billion in 2018 program payments (72% of Medicare Part A’s $190.7 billion spend). Although this is a fee-for-service payment structure, hospitals are still financially incentivized to meet certain quality thresholds through programs such as Medicare’s Hospital Readmissions Reduction Program, which penalizes hospitals for high 30-day readmission rates.
Key revenue drivers for startups serving the hospital market are: reducing readmission rates, decreasing average inpatient length of stay and increasing patient satisfaction. Contessa Health and Medically Home are companies leading the charge of allowing patients to receive hospital-level care at home (“Hospital in the Home”).
CMS recently announced new guidance for coverage of these services that allows hospitals to meet their quality and payment goals, especially in a COVID-restricted environment. The best companies will be able to precisely quantify their value creation for the customer, whether that be the hospital or the payer contracting for these services.
SNFs are the second largest provider of Part A services, obtaining $28 billion in 2018 program payments (15% of Medicare Part A spend). Medicare requires a patient to spend three consecutive days in inpatient care at a hospital to receive Part A coverage for a subsequent SNF stay. CMS recently updated SNF reimbursement models, incentivizing SNFs to prioritize patient needs, particularly patients’ with complex care, over service volume.
An emerging category of startups is building and serving Institutional Special Needs Plans (I-SNP). I-SNPs are special MA products for patients who are likely to spend more than 90 days in a facility (e.g. a SNF) in a given year. Startups can serve these plans by improving enrollment and helping plans deliver high-quality, cost-effective care in the facility. Longevity Health Plan and Ally Align are companies that are partnering with SNFs to co-locate medical and residential services through I-SNP products.
naviHealth, recently acquired by Optum, built a large business managing patient transitions of care from hospital, to SNF, to home through proprietary decision-support technology that leverages data collected at multiple points throughout a patient’s journey. Patient Ping and Post Acute Analytics are both early stage companies gaining traction using automated data capture and predictive analytics to improve continuity of care between acute and post-acute episodes of care.
Several startups help SNFs optimize care by leveraging telehealth services. Tembo Health and Arkos Health (created through merger of Curavi, CarePointe and US Health Systems) help SNFs achieve quality goals and reduce readmissions by introducing otherwise inaccessible specialist physicians through telehealth. These startups help reduce inpatient hospitalizations through telehealth visits, an example of the decade-long cost-shifting we’ve seen between Medicare Parts A and B.
HHAs are other post-acute care providers that play a large role in transitions of care between acute and post-acute care through home-based nursing care. The home health industry is quite fragmented, with over 12,000 agencies contracting with Medicare to deliver services to beneficiaries.
A few companies, like PE-backed CareCentrix, work closely with MA plans to standardize and streamline the quality and outcomes of home health networks. In addition, Honor, which has raised over $255m in total funding, works closely with independent HHAs to streamline front- and back-end systems. The company also works closely with their agency partners to assist in staffing for home health nurses.
The home health industry is one that broadly struggles with high turnover rates and a wide variation in quality of delivered services. We anticipate many more early stage companies will enter this market to better manage the $18 billion Medicare pays to home health companies in Parts A and B.
Medicare Part B
Startups innovating in the Medicare Part B space are reshaping the delivery of medical care and supplies provided in the outpatient setting. In particular, startups are focusing on telehealth, alternative sites of care and access to durable medical equipment.
In recent years, CMS has expanded telehealth services covered by Medicare, including wellness visits, psychotherapy, diabetes self-management training services and more. More recently, CMS further expanded telehealth coverage to treat COVID-19.
Traditional telehealth players are responding to these new incentives. For example, Doctor On Demand became the first nationwide telehealth provider to expand its services to include Part B coverage and offer telehealth medical services to the 33 million Part B beneficiaries in response to the COVID-19 pandemic. In March, their registrations for the 65-and-over age group grew by nearly 150%.
Other telehealth startups focus on specific health conditions. For example, Forefront Telecare offers virtual behavioral telehealth to seniors in hospitals, long-term care and home health settings. In addition to providing telehealth services, companies like early stage Doxy.me and recently IPO’d American Well, can serve as telehealth technology platforms that allow any healthcare provider to provide telehealth care to their patients.
As noted earlier, several companies are working to shift medical care historically delivered in acute care settings into the home. Two notable companies providing on-demand, clinical-grade care in the home are Dispatch Health and Heal. These companies have the ability to bring the necessary equipment to treat patients in their homes for both urgent and primary care health needs.
Other VC/PE-backed companies, such as Landmark Health and Concerto Health, have established longitudinal home-based primary care and care-coordination programs for interdisciplinary care of the highest medical risk populations.
In addition to care delivery, a few companies support Part B-covered supply delivery, namely medically necessary durable medical equipment (DME). Parachute Health works to streamline DME fulfillment processes by allowing DME suppliers and ordering providers to collaborate in real time, automating CMS-mandated documentation and ensuring patients receive the appropriate DME to improve patient outcomes.
Tomorrow Health, is an example of an early stage company that has chosen to serve as a fully contracted and credentialed DME provider. By going through the necessary Medicare supplier contracting rules, the company is looking to improve cost and service offerings for payers, providers and ultimately patients.
As covered in Part 1 of this article, the drugs covered under Part B are high cost and strategically important, since they can be purchased through the 340B Program. The 340B Program can be quite profitable for providers who can "buy and bill" these drugs and retain profit margin as a result of the discounted 340B cost.
Some early stage companies have entered this marketspace to help provider groups navigate this dynamic market. Trellis Rx is a company that partners with health systems to fund, build, and grow patient-centered specialty pharmacy programs under their partners’ brand. Kalderos, which recently raised a $28 million Series B round, delivers a SaaS-based drug-discount-management solution that identifies, checks and resolves 340B rebate payments.
Medicare Part C
Many of the startups introduced thus far that serve Medicare Parts A and B can also serve Medicare Part C (also known as MA plans). MA plans offer managed care versions of the same components in Original Medicare – Part A (acute and post-acute care) and Part B (outpatient care, DME, some drugs).
MA plans can also manage the Part D prescription drug benefit. MA plans have more latitude than FFS Original Medicare to structure value-based contracts incentivizing providers and vendors by sharing “financial risk” to deliver innovative solutions to covered populations.
Companies operating in the MA sector are often seen as the most innovative within the Medicare market because of an emphasis on value-based care. These companies can function in a variety of ways, but we’ll focus on companies delivering value-based care directly to patients, helping existing primary care providers transform into value-based care models and addressing social determinants of health. Finally, there are a few startups competing directly with incumbent MA plans by starting their own de novo innovative MA plans.
An important class of emerging companies serve as risk-enablement platforms to help primary care practices that serve Medicare patients move toward value-based care. For physicians treating Medicare patients, especially those in private practice, it can be challenging to identify vendors offering validated, innovative services.
Startups like Agilon, Aledade, VillageMD and Stellar Health offer providers access to data, technology and personalized practice transformation services to succeed in risk-bearing MA contracts. Startups entering the MA market can serve as risk-enablement platforms themselves or can partner with these existing platforms to deliver world-class solutions to the provider practices many of these companies represent.
Given the slow pace of adoption of value-based practices by legacy providers, several earlier stage companies have found success by serving as full stack Medicare-focused primary care clinics. These startup providers have designed innovative care delivery models that align with MA’s value-based model.
For example, Iora Health (a Flare Capital company), Oak Street Health (which recently closed a very successful IPO) and ChenMed are all growing platforms with national reach that deploy team-based primary care models that integrate high-touch care for Medicare beneficiaries.
While many of these primary care startups partner with MA plans, some startups in the Part C space launch as health plans themselves. These startup MA plans, including Bright Health (a Flare Capital portfolio company), Devoted Health, Alignment Healthcare and Clover Health, are responding to MA’s growing enrollment, which is projected to continue growing and reach 47% of all Medicare beneficiaries by 2029. This new class of MA plan often deploys a mix of tech-enabled health plan and provider capabilities to ensure their members receive cost-effective, comprehensive healthcare.
Supplemental Benefits and SDoH
Supplemental benefits and the social determinants of health (SDoH) are areas where CMS has continued to innovate in how MA plans operate. Supplemental benefits are defined as additional services not covered by Parts A, B or D, but ones that promote health and wellness. An important differentiator of MA plans from Original Medicare is the ability to provide coverage for the supplemental benefits. The most widely utilized examples of supplemental benefits are vision, hearing and dental benefits, with nearly 90% of all MA plans offering these in-demand benefits.
An emerging class of supplemental benefits has become known as SDoH. These are “non-healthcare” related benefits that can still impact health through modifying a beneficiary’s living environment. More importantly, the availability of these resources in one’s community ties closely to socioeconomic status, and thus significant disparities exist across diverse populations. Examples include food insecurity, in-home support and transportation to clinical visits. MA plans increasingly have flexibility to cover these non-healthcare supplemental benefits, particularly for their chronically ill beneficiaries, through MA’s capitated payment model.
There are a growing number of digital health companies beginning to work with MA plans to enable beneficiary access to SDoH. Several companies serve as aggregators, such as Unite Us, Healthify and Signify Health, who will assess member needs and curate networks of SDoH suppliers such as food pantries and housing assistance groups. Given the diffuse nature of the community benefit organizations that provide access to SDoH, these aggregators are also tasked with attempting to close the loop and ensure fulfillment of services.
There are also a growing number of companies who may focus on a particular SDoH, such as nonemergency medical transportation or food insecurity, and become vendors of those services. Examples of these companies include CareCar, SafeRide and Circulation Health (a Flare Capital company acquired by Logisticare), all of which have partnered with MA plans.
With the advent of COVID-19 and the deleterious impact on the economy, food insecurity is at an all-time high. In response, over 50% of MA plans now have some form of coverage of nutritious meals. Each MA plan may have different criteria for which beneficiaries receive coverage, since most plans will cover meals for patients recovering from certain illnesses or managing uncontrolled diabetes. As coverage for meals grows, we anticipate several early-stage startups will rush in to manage this potentially expansive benefit.
Star Ratings system
To assess and reward quality for Medicare Part C and D plans, CMS uses a “pay for performance” program known as Star Ratings. Plans are rated on up to 45 unique quality and performance measures, such as colon cancer or osteoporosis screening rates. The Stars scale ranges from a low of two stars to a high of five stars, with plans at or above four stars eligible for millions of dollars in quality bonus payments (QBPs).
Through the Stars system, CMS created an incentive-laden program MA plans closely adhere to. In 2020, more than 80% of MA beneficiaries were in a four-Star plan or higher, suggesting one metric of success of the program. Early stage companies able to demonstrably impact Stars ratings can make a strong ROI case and potentially share in this quality-driven value creation.
Medicare Part D
Part D, Medicare’s $95 billion prescription drug benefit, is an area where some medication management startups are starting to focus. A key component of Part D is Medication Therapy Management (MTM) programs, which reimburse providers to deliver additional medication management/adherence services to patients with complex health needs. In addition to supporting medication adherence, which we’ve written about extensively, other areas of focus include disrupting traditional pharmacy distribution models, redesigning prescription practices and supporting medication therapy management.
Startups disrupting traditional pharmacy models are launching as in-network pharmacies reimbursed by Part D plans. New pharmacy models focus on reducing barriers to access and adherence for prescription drugs. For example, PillPack (acquired by Amazon) offers patients free delivery for prescribed medications, organizes pills in blister packs by date and time of administration, automatic refills, and pharmacy support, all at no additional cost beyond the patient’s regular co-pays.
While much of the innovation happening in pharmacy is directed towards commercial consumer populations, there are a few companies, like RxAnte, that have long been focused on higher-needs Medicare populations. RxAnte, a previously VC-backed startup that has been through a few M&A transactions, has been long focused on delivering medication adherence analytics to MA plans.
The company recently entered the pharmacy distribution space with Mosaic Pharmacy Service, an offering that delivers analytics-enabled care management, in-home care and medication delivery to medically complex and vulnerable Medicare beneficiaries.
Instead of launching as a new pharmacy service, other startups enable existing pharmacies and MA plans to better serve their patients and beneficiaries. Digital Pharmacist serves pharmacies directly by offering patient communication and management tools as well as digital marketing. Aspen RxHealth (a Flare Capital company) partners with MA plans and creates a “gig economy” platform that connects pharmacists directly to patients to deliver MTM services, as well as a handful of other value-added pharmacist-led interventions, to ensure appropriate medication usage.
Other startups redesign prescription practices to improve patient adherence and reduce costs. For example, RxRevu integrates real-time, customized cost information, coverage restrictions and therapeutic alternatives into providers’ EHR workflows. The company also offers behavioral analytics to reduce care variability, improve patient safety and better manage pharmacy risk.
We anticipate a number of startups will continue to enter the Part D market space to power Medicare beneficiary consumer decision-making. Medicare beneficiaries have medication regimens costing more than $3000 per year with various forms of cost sharing. Further, many Medicare beneficiaries surveyed suggest the Part D formulary is a major decision factor when subscribing to an MA plan. We anticipate MA plans will invest significant dollars to ensure beneficiaries have a world-class prescription drug experience.
Medicare coverage for specific conditions
In addition to Medicare Parts A through D covering hospital, medical and drug insurance, there are other programs uniquely reimbursed by Medicare that startups can address. We highlight three programs launched by the Center for Medicare and Medicaid Innovation (CMMI) addressing medical conditions ripe for innovation: end-stage renal disease (ESRD), oncology and hospice.
End-stage renal disease
Over 37 million individuals in the U.S. live with chronic kidney disease (CKD), and over 700,000 Americans have ESRD requiring dialysis treatment. As noted in Part 1 of this article, ESRD became a Medicare-covered benefit in 1972 when President Nixon added an amendment to the Medicare law. Although ESRD beneficiaries comprised less than 1% of the Medicare population in 2016, the $35.4 billion in total medical spending for this population accounted for over 7% of total Medicare expenditures. Currently, only 12% of patients receive lower cost, home-based therapies such as peritoneal dialysis and home hemodialysis. In addition, the transplant waitlist process is archaic and inefficient, with average waitlist times of five years. Kidney transplant is truly a life or death proposition as ESRD without a transplant carries a 20% one-year mortality rate, and a 65% five-year mortality rate.
To address high costs and treatment inefficiencies associated with kidney care, CMMI recently developed new ESRD payment models that prioritize home dialysis and address transplant rates. In addition, the 21st Century Cures Act will lift the current restrictions preventing individuals with ESRD from enrolling in MA plans effective 2021. CMS estimates that an additional 83,000 people with ESRD, representing a 63% increase, will enroll in MA plans through 2026.
Many MA plans that have not previously managed populations with ESRD and late-stage CKD have looked to early-stage companies to assist them in managing this high-need, high-cost population. An example is Somatus (a Flare Capital portfolio company), which works closely with health plans and risk bearing providers to deploy field-based nursing teams to manage populations while leveraging advanced predictive analytics and risk stratification to manage healthcare utilization and dialysis networks to ensure lower cost, high-quality outcomes. Given the immense need of this market, several other VC-backed companies such as Strive Health, Monogram Health and Cricket Health have also similarly moved in to help manage this population.
Oncology
Over 1.6 million people are diagnosed with cancer each year in the U.S., with 54% of new cancer cases occurring amongst Medicare beneficiaries. With total cancer costs in the U.S. projected to be over $173 billion in 2020, Medicare shoulders a large burden bearing approximately one-third of these costs.
To improve quality of care outcomes and lower costs for this medically complex population, CMMI has developed a new Oncology Care Model (OCM). OCM provider participants receive augmented payments from CMS in two forms: a monthly payment of $160 per-beneficiary, per month to deliver OCM-enhanced services and a performance-based payment for OCM Episodes.
Through these performance-based payments and reformed delivery models, the OCM aligns financial incentives to improve care coordination and appropriateness of care for Medicare patients receiving chemotherapy. Startups, including Integra Connect and Tuple Health, are supporting OCM participants in achieving these goals by offering deep data analysis, redesigned care management infrastructure and other services to support OCM providers in their value-based journey.
Although there is significant promise in the ability to move oncology care into the world of value-based assessments, the lucrative nature of provider billed rates for cancer medications will provide some inertia. One study found that practices in only 37% of markets participated in the OCM. Further, the data suggests that oncology practices without significant competition were less likely to participate in value-based programs. We anticipate startups will continue to enter this marketspace and iterate on novel incentive driven models to deliver value to key stakeholders.
Hospice
Hospice is a team-based approach to care for patients expected to be within the last six months of life. More than 95% of hospice care is delivered in the patient’s home to ensure comfort and prevent hospitalization. Hospice has traditionally been covered by Original Medicare under Part A, generating $19.3 billion in program payments and serving 1.6 million Medicare beneficiaries in 2018. The hospice market has been a lucrative one for many independent home and hospice companies, who can receive up to $5000 per month for hospice services delivered to patients within the last six months of life. An industry that has changed little since the benefit was established in the 1980s, it has faced questions of fraud, waste and low utility.
In a situation similar to that of kidney care, to better manage hospice costs CMS is preparing to allow MA plans to manage the lucrative benefit. After a lengthy comment period, CMMI will launch the MA hospice benefit “carve-in” demonstration beginning January 1, 2021. MA plans for the first time will have the ability to manage costs associated with patients who have elected hospice care in the last six months of life.
There have been relatively few early-stage startups who have gained significant traction in managing Medicare beneficiary care near the end of life. One notable exception was Aspire Health (acquired by Anthem), which partnered with MA plans and provider practices to deliver community based interdisciplinary palliative care. Palliative care – which is care designed to help patients and families navigate serious Illness management through symptom management while addressing goals of care and managing advanced directives – is seen as a natural precursor of hospice care, and has been associated with improved quality and reduced costs for patients nearing the end of life.
We anticipate a few startups will enter the hospice management marketspace as the industry begins a decade-long shift into value-based care. We foresee significant value creation opportunities in tying the current $20 billion of spend to improved quality outcomes and higher value, lower cost care for this population near the end of life.
Key aspects of winning models
Based on our survey of the Medicare landscape, we offer five recommendations for launching startups in the Medicare space.
1. Develop solutions with an eye towards MA and value-based care. Although startups’ services and products may be reimbursed by both Original Medicare and MA, the latter still offers greater incentives to innovate value-based care solutions due to its reimbursement model. Many of the startups we featured that serve fee-for-service Medicare players also serve MA plans. MA enrollment is projected to continue growing and CMS continues to launch more value-based programs.
2. Explore delivery models outside hospitals and traditional clinics, especially in-home health. While hospital care is reimbursed by Medicare Parts A and C, startups are increasingly disrupting traditional care delivery by addressing gaps in transitions of care to post-acute settings, SDoH and other areas that hospitals and traditional clinics have yet to address themselves. These areas often align with value-based models and financial incentives.
3. Track CMS rules and regulations and be agile in pivoting to take advantage of updates. While it can be challenging to predict policymaking, market spaces with disproportionately high spending are often subject to regulations that seek to align financial incentives with quality, cost-effective outcomes. Examples include ESRD, oncology and hospice, among other areas. To better understand where the policy “puck” is heading, startups can participate in industry-specific conferences and get involved with policy groups that spend dedicated resources in reporting on and influencing CMS regulations (e.g., Kaiser Family Foundation, The Commonwealth Fund, Better Medicare Alliance). Alternatively, early-stage companies can invest in advisors or regulatory consultants who closely follow regulatory cycles and key policy makers, and can provide opinions in real time.
4. Recognize traditional cost shifting between Medicare industry players and identify opportunities to create value. Healthcare cost savings rarely occurs in a vacuum. There is an interconnected web of providers and suppliers all vying for healthcare dollars. Practically, to remove costs from one low-value service line, payers shift costs to a “higher value” provider, with the hopes that quality is maintained or improved. Startups can create value for industry players by anticipating the highest value site of care through analytics, improved targeting and patient navigation, and offering supplemental benefit needs through other non-medical interventions.
5. Focus on the beneficiary, in the context of increasing consumerization of healthcare. Medicare beneficiaries are a primary driver of adoption: they have skin in the game through out-of-pocket payments and CMS is increasingly empowering beneficiaries with transparency tools for consumer decision-making. Most importantly, if startups aren’t able to drive adoption from beneficiaries, there won’t be value creation. Therefore, startups must design patient centered solutions that engage beneficiaries and be able to demonstrate consumer buy-in when partnering with providers, payers and other clients.
Conclusion
We believe the Medicare market is ripe for innovation and contains several untapped value creation opportunities for early stage companies. To gain traction, startups should be deliberate in understanding reimbursement rules and regulations that govern management of the $750 billion of total Medicare healthcare spend. Further, startups will have a higher likelihood of success if they partner with experienced operators, advisors and investors who have had success in Medicare-oriented businesses. We believe these collective teams of innovators can navigate the requisite financial incentives and regulatory hurdles to deliver world class healthcare to millions of deserving beneficiaries.
About the authors
 Gwendolyn Lee is a member of the 2020 Flare Capital Partners Scholars program. While completing her MPP at Harvard Kennedy School, she interned at the Massachusetts Health Policy Commission and the Massachusetts eHealth Institute. She is currently a third-year medical student at the David Geffen School of Medicine at UCLA.
Gwendolyn Lee is a member of the 2020 Flare Capital Partners Scholars program. While completing her MPP at Harvard Kennedy School, she interned at the Massachusetts Health Policy Commission and the Massachusetts eHealth Institute. She is currently a third-year medical student at the David Geffen School of Medicine at UCLA.
 Dan Gebremedhin, MD (@dangebremedhin) is a partner at Flare Capital Partners, a Healthcare Technology and Services-focused VC Firm. Prior to Flare Capital, he served as a practicing physician at the Massachusetts General Hospital, a medical director at the Harvard Pilgrim Health Plan and an entrepreneur in the health IT industry.
Dan Gebremedhin, MD (@dangebremedhin) is a partner at Flare Capital Partners, a Healthcare Technology and Services-focused VC Firm. Prior to Flare Capital, he served as a practicing physician at the Massachusetts General Hospital, a medical director at the Harvard Pilgrim Health Plan and an entrepreneur in the health IT industry.


















